This case takes place in California and involves a delayed diagnosis of blood clots causing complications. The patient presented to the ER with symptoms of pain, nausea, and difficulty walking. The patient was initially treated with pain medication and intravenous fluids. The patient was seen by the defending doctor, who made notes indicating the patient was not in pain and appeared to have full mobility, although she remained in pain and was not ambulatory. The doctor discharged the patient from the ER with a diagnosis of dehydration. Several days later, the patient’s pain and immobility continued, and she went to get a second opinion. The physician saw her and at once suspected acute compartment syndrome. The physician made a call to another physician regarding her condition and she agreed that the patient was suffering from acute compartment syndrome and required immediate surgery. The patient was sent back to the emergency room for a CAT scan, which revealed that the patient had blood clots in her legs, believed to be caused by an autoimmune onset of Antiphospholipid Syndrome.
Question(s) For Expert Witness
1. How often do you treat patients with these presenting complaints?
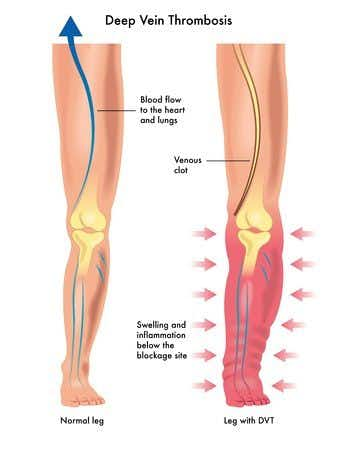
2. What are the steps to rule out blood clots or Acute Compartment Syndrome?
Expert Witness Response E-008184
In my 30 year career as an emergency physician, I have seen many thousands of patients with a complaint of extremity pain. Of those, I have probably seen close to 100 patients with an actual diagnosis of either DVT or compartment syndrome. The steps to rule out either blood clots or acute compartment syndrome depend upon the clinical suspicion for those diagnosis. If clinical suspicion based on history and physical exam is low enough, no further testing is required. As clinical suspicion rises, the need for more definitive testing also rises. For DVT, testing can include any or all of the following: dimer blood testing, various types of ultrasound, CT/MTI or nuclear medicine imaging. For compartment syndrome the same general principles apply, in which various blood tests, or various imaging can take place. An invasive measurement of the concerning compartments can also be made. If clinical suspicion is high enough, the patent can be directly taken to the OR without any further testing. What the standard of care would be in this individual case would depend upon the specifics of this case as described in the medical record and further amplified in deposition of the involved parties.

About the author

Joseph O'Neill
Joe has extensive experience in online journalism and technical writing across a range of legal topics, including personal injury, meidcal malpractice, mass torts, consumer litigation, commercial litigation, and more. Joe spent close to six years working at Expert Institute, finishing up his role here as Director of Marketing. He has considerable knowledge across an array of legal topics pertaining to expert witnesses. Currently, Joe servces as Owner and Demand Generation Consultant at LightSail Consulting.

