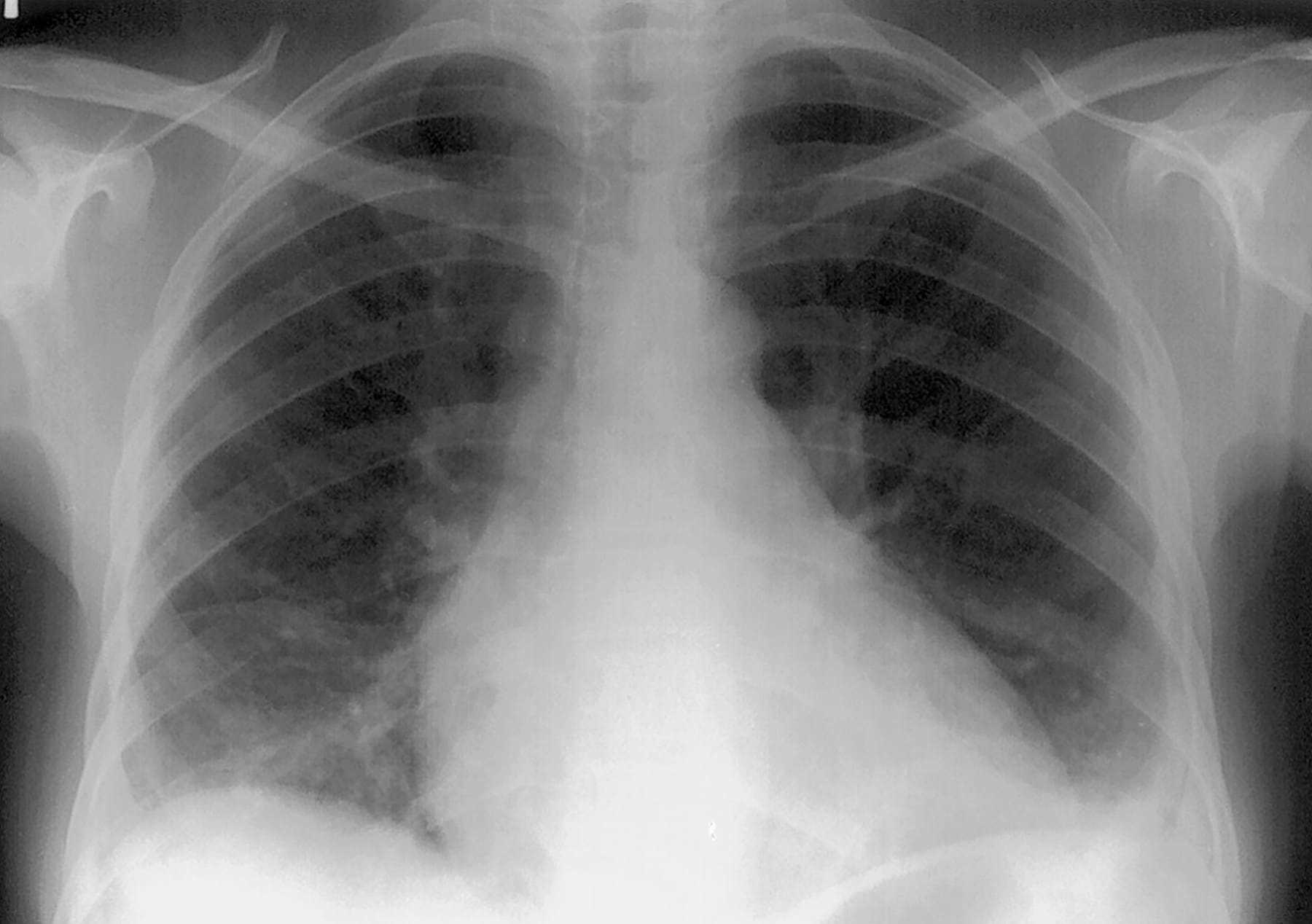
This case involves a sixteen-year-old male who presented to the ER with fever, cough, shortness of breath, and intense chest pain. The boy’s past medical history included sickle cell anemia and recurrent infections. An x-ray was performed and he was diagnosed with pneumonia. Antibiotics and intravenous fluids were administered to him for a day. The next day the patient’s oxygen saturation declined to 65% and he still experienced fever and chest pain. He was given pain medications and received continuous positive airway pressure (CPAP). His oxygenation level continued to decline until he lapsed into a coma. After being resuscitated for twenty minutes, the boy regained consciousness. Once stabilized, it was evident that he sustained brain injuries as a result of oxygen deprivation. He was discharged once he was able to breathe independently. The months following hospitalization, the boy was unable to perform rudimentary tasks such as feeding and dressing himself, and formulating clear sentences. His teacher reported that his reading and writing level was at a third-grade level and he was unable to keep up with his peers. He required homeschooling, occupational therapy, and physical therapy. His pediatrician noted that he believed the boy experienced acute chest syndrome. This diagnosis was not made by the ER.
Question(s) For Expert Witness
1. Did the emergency medicine team properly manage this boy’s symptoms, and what could have been done to prevent the damages that occurred with this patient?
Expert Witness Response
This emergency medicine team failed to make the diagnosis of acute chest syndrome, a serious complication of sickle cell anemia. Acute chest syndrome is a condition within the pulmonary vasculature that results from deoxygenation of hemoglobin. This deoxygenation causes the blood to sickle and occlude these vessels. Patients aged ten to nineteen will most commonly develop acute chest syndrome after an infection. The diagnosis is based upon the presence of a new pulmonary infiltrate with chest pain, temperature > 38.5 degrees Celsius, tachypnea, wheezing, cough or increased work of breathing, and hypoxemia. Due to the seriousness of this condition, this boy should have been monitored more closely. This patient was properly managed with intravenous fluids, antibiotics, pain medications, and respiratory assistance. However, exchange transfusion was never put in place. This intervention is critical because it addresses the most serious complication of this syndrome; hypoxemia. Prolonged hypoxemia in this case resulted in permanent neurologic damage. This could have been avoided had the transfusion been initiated.

About the author

Stephen Gomez, J.D.
Stephen Gomez, J.D., is the General Counsel and Corporate Secretary at Lumos Labs, where he oversees legal and compliance matters in areas like privacy, intellectual property, and litigation. He has extensive legal experience in the e-commerce, media, and entertainment industries, previously holding key roles at Thirstie, Equinox Media, and SeatGeek. Gomez also contributed to legal functions at HelloFresh and Chubb and has a background in legal content and research management. He earned his J.D. from Boston University School of Law and a B.A. in Politics from New York University. His expertise lies in providing strategic legal advice to fast-growing companies.

